
How to leverage low hanging fruit for long term lean success
FEATURE – The importance of leveraging early successes to drive engagement to lean is often talked about. The story of this Brazilian hospital confirms this is the way to go.
Words: Aline Augusto Ribas, Laura Friggi Peters de Holanda, Lin Hung Hua, Maria Cristina Pose Guerra, Marilisa Silva Diego, Otávio Lima de Holanda, Renata Mantovani; SPDM - Hospital Municipal Dr. José de Carvalho Florence - Brazil
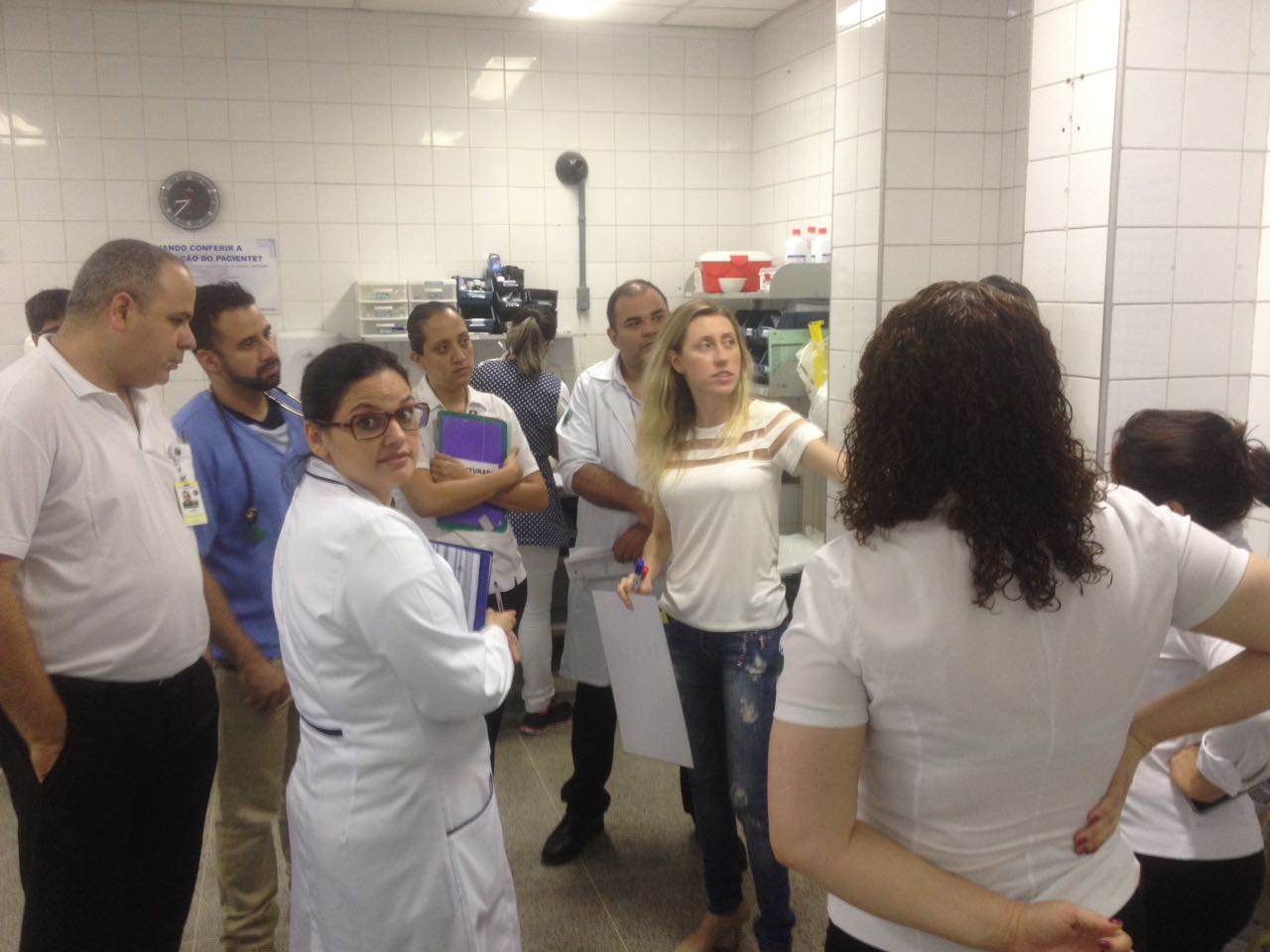
There is a lot of talk about where and how to start a lean transformation, but what seemed very clear to us from the onset was that the best way to begin is by tackling a problem that everybody is aware of. For us at the Hospital Municipal Dr. José de Carvalho Florence (a 400-bed public hospital in São José dos Campos, in Brazil), that problem was the Emergency Room.
Our Pronto Socorro is incredibly busy: we receive between 800 and 1,200 people every day (for a monthly average of 20,000). There is never a dull moment in our ER, which is why it’s important it works as efficiently and effectively as possible.
There were two main problems the ER was experiencing, and – like for most other hospitals in the world – they both had to do with the number of patients we see and the amount of time they spend with us: on the one hand, we realized the length-of-stay of our low-to-medium priority patients (together, they represent over 90% of the people we see – their color codes are respectively “blue/green” and “yellow”) was excessive and (our second issue) that our Observation Room was constantly bursting with patients waiting to be visited.
We decided to use lean thinking to tackle these issues. The impact the methodology has had on the quality of care our patients receive (and on the working life of our staff) is hard to understate. We hope – and think – this is just the beginning of a transformation for the whole of the organization.
But let us tell you about these two problems, and how we successfully solved them.
“YELLOW PATIENTS”
Discharging our low-priority patients had become one of our hospital’s biggest challenges: “yellow patients” (which refers to the color code we use for them) spent anywhere between three and twelve hours with us, which frustrated them, overburdened our staff and increased clinical risk.
Interestingly, the bottleneck was not at the examination point. People had no particular trouble reaching the hospital and seeing a doctor, but it took them a very long time to receive the medication they needed. Since 40% of our ER patients need to be given drugs, this of course created massive discharge delays.
Further analysis revealed that one of the root causes of the problem was the long distances our patients had to travel within the hospital every time they had to be given drugs: there were 277 meters between the emergency care unit and the medication room. People walked without knowing where to go and asked for directions all the time – imagine the confusion! In turn, the excessive movement created batches at the point of patient reassessment. We also observed great variability in the way we administered drugs to our patients.
The countermeasures we identified through PDCA were:
- Improving patient flows by changing the department’s layout; and
- Improving care by introducing standards in the way we treat patients.

The first push towards using lean thinking to solve these issues actually came from the Board (as a public hospital, we don’t have a lot of resources – which is why lean immediately appeared as a very attractive approach), which was concerned about the excessive length-of-stay and asked us to tackle it as soon as possible. The problem in our ER must have been really evident to our people, however, because we didn’t experience the resistance that lean initiatives are commonly met with at first. People got on board pretty quickly, because they immediately saw the value in what we were trying to do: we all thought it was unacceptable that our patients had to walk that far just to get medication, especially considering that, by definition, these are people in pain and distress.
Our decision to change the layout and move the Medication Room closer to the Examination Area, which came from our use of spaghetti diagrams and value stream maps, had two immediate results: first, it greatly reduced movement (and therefore chaos and the chance of mistakes being made) and, secondly, it allowed us to introduce a “single-patient flow” – thus speeding up the reassessment process and, naturally, discharge. The distance our patients have to cover now is 40% shorter, the ER is visibly less crowded, and the number of people wandering around and asking for directions has dropped.
On to the second problem.
By means of a Pareto analysis, we determined that 70% of our patients had pain-related conditions, while around 10% showed up with asthma. Upon reviewing our protocols for administering drugs to these two categories of patients, we realized that we didn’t have a standard for treating them. Many of our pain patients were being given drugs via an IV, even though oral drugs – which make for a much quicker administration and, therefore, no bottleneck – are just as effective. Therefore, our new protocol for patients with pain favors oral drugs and entails giving patients the medication they need to continue treatment at home for a couple of days, so that they don’t need to come back in straight away.
As a result, in the first month, we had 1,500 less patients visiting the Yellow Area. (We expect the impact of the new asthma protocol to become more evident soon, as our winter has just begun.)
These changes weren’t necessarily easy to introduce: changing the layout of the ER was a labor-intensive and difficult process, as was convincing our doctors to follow the new protocols. We can’t stress enough how instrumental our early adopters were in getting the rest of the team on board: we have certainly learned how critical teamwork is when trying to implement lean change.
We have also seen the importance of testing our countermeasures and learning from the mistakes we make. Overall, however, the impact of lean in the ER couldn’t be clearer: average length-of-stay for yellow patients has gone from 3 hour and 24 minutes to 1 hour and 55 minutes.
DAILY HUDDLES
As mentioned earlier, another huge problem – perhaps the most critical – the ER of the Hospital Municipal was experiencing was an overcrowded Observation Room, which at times held twice as many people as it could.
The bottleneck was the result of a number of problems resulting from our poor process: for example, our doctors took too long to reassess patients and our tests took too long to become available or be checked. Patients, who had to face long waits to see a specialist, were rightly dissatisfied and often had to remain in the ER after being discharged, because wards had no space to admit them.
Our processes were slow and clunky. Very often, a doctor would go to a room to see a patient and wouldn’t know another one was also there, ready to be visited. In addition, it was not always clear what doctor should see what patient, there was no clarity over hand-overs, and realizing a patient’s condition was deteriorating wasn’t always possible because everyone was so busy all the time.
To try and simplify, we can say our difficult situation stemmed from two main root causes: a poor flow of communication and a lack of coordination among professionals. If you keep this in mind, it won’t be surprising for you to hear that the countermeasure we decided to adopt is one of the most popular “lean inventions” available to practitioners: the daily huddle. Their positive effects on communication and collaboration among professionals and teams are well known, and now we can vouch for them ourselves.
Our project aimed at improving the quality of care, reducing clinical risk, variability and the burden on our people. But as the old lean adage goes, you can’t improve what you can’t measure. This is what ultimately makes the daily huddles so important to us: they allow us to know everything we need to know about the daily work.
Our first daily meeting took place in November 2016 and felt very strange: it took way too long because we had no idea what we were doing and none of the information we needed was ready. A few days later we started to get the data earlier, before getting into the huddle, and over time – by continuously applying PDCA – we changed the questions to make them more effective.
Currently, during our 8.30 AM huddle, we ask each other how many patients are ready for discharge or final assessment on any given morning. We also ask how many exams are pending and why, and how many patients are ready to go but can’t be transferred to the wards yet (which is a cue for us to notify other departments that we need a bed soon) or are still waiting for a relative or ambulance to pick them up. Everything is based on a red/green color code, which means we know immediately where problems are and which ones we need to tackle first.
As part of our work to ease the pressure on our Observation Room, we have also implemented visual management. Prior to this, doctors arrived in the room and didn’t know exactly what patients they had to see. This encouraged them to create tags for patients, which are now placed on beds.
It took a few experiments, but we eventually got it right. Below, you’ll see an example of a tag, in which the eyes mean the patient is not ready to be admitted to a ward yet, the food sign that he is not to eat anything, the thumbs-up that the exams are ready and awaiting the doctor’s decision. You can also see the department that will take care of the patient (in this case, CG stands for General Surgery) and the bed number.

We can’t say the daily huddles are standard behavior yet, but that’s understandable considering we have only been doing them for six months. Still, our people can clearly see that things are running more smoothly already, and the daily meetings have started to take place even when the leaders are not around. In fact, we have launched two more huddles, one in the late afternoon and one late at night (the Observation Room changes dramatically over the course of the 24 hours).
The results are already here: our process is more stable, and not only have we been able to lower the number of patients that visit the Observation Room daily by 40%, but we have also decreased the amount of time they spend there.
We have also noticed how people are trying to arrive at the huddle without any problems to report (the meeting clearly functions as an incentive to fix issues as soon as they appear). Critically, we now have visibility over the work to be done for each patient and know exactly what information we need to make our decisions. It is hard to make mistakes when you have all the information laid out in front of you (it’s great to see, for example, how unlikely it has become that a critical patient gets overseen).
WHAT’S NEXT?
We believe these two projects – which have taken place simultaneously – have laid the foundations for our lean work to spread to other parts of the hospital. By launching the huddles, for instance, the team has already come to the conclusion that they will need to involve people from other departments if they are to have all the information they need on a daily basis.
Even though they started as a top-down initiative, we were delighted to see how impactful these two projects have been: they benefitted everyone – from patients to employees – and inspired others to also embrace change. We are now trying to get more people on board, building on the momentum that the improvement of our ER has generated.
Stay tuned, this is not the last you hear of us.
THE AUTHORS

The Emergency Department team who wrote this article:
Aline Augusto Ribas, Administrative coordinator
Laura Friggi Peters de Holanda, Medical ER coordinator
Lin Hung Hua, Medical director
Maria Cristina Pose Guerra, Nursing director
Marilisa Silva Diego, Administrative manager
Otávio Lima de Holanda, Doctor
Renata Mantovani, Nursing Coordinator
Read more

FEATURE – This time of crisis is a perfect opportunity to use Lean Thinking to review processes, improve standards and prepare ourselves for the “reconstruction”, says Sharon Visser.

CASE STUDY – How do you give hundreds of primary care units the tools and knowledge they need to make improvements? The Catalan Health Service found the solution in hoshin kanri.

FEATURE – Philips has embarked in an ambitious development program for lean executives, which is helping the organization make substantial progress in their transformation.

CASE STUDY – A very lean system that runs like clockwork and constant attention to customer service enable Barcelona-based 365.café to achieve the impossible: supplying 55 bakeries out of a 650-sqm factory.